Chapter 5: Community Improvement Planning

Vocabulary List
(Merriam-Webster, 2023)
Bigotry: obstinate or intolerant devotion to one's own opinions and prejudices: the state of mind of a bigot.
Competence: the quality or state of having sufficient knowledge, judgment, skill, or strength (as for a particular duty or in a specific respect).
Dissemination: the act or process of disseminating or spreading something.
Ecological: relating to the environments of living things or the relationships between living things and their environments.
Ethical: conforming to accepted standards of conduct.
Harassment: to create an unpleasant or hostile situation, primarily through uninvited and unwelcome verbal or physical conduct.
Obligated: to bind legally or morally.
Prevalent: generally or widely accepted, practiced, or favored.
Privacy: freedom from unauthorized intrusion.
Racism: a belief that race is a fundamental determinant of human traits and capacities and that racial differences produce an inherent superiority of a particular race.
Segmentation: the process of dividing into segments.
Vulnerable: capable of being physically or emotionally wounded.
Introduction
This week, you will learn about the most common planning models employed in developing programs for public health. These models will serve as the basis for a practical experience exercise in creating a community health program.
W05 Study: Eight Areas of Responsibility
Notice: Public health deals with health on a population level.
The National Commission for Health Education Credentialing (NCHEC) identified the following competencies for Health Educators (NCHEC, n.d.).
A critical role in public health is the health educator.
Eight Areas of Responsibility
(National Commission for Health Education Credentialing, Inc., n.d.)
Area I: Assessment of Needs and Capacity
- Obtain data and analyze it to prioritize the health needs of a population.
Area II: Planning
- Assemble partners, develop specific and time-bound objectives, and create a logic model.
Area III: Implementation
- Deliver the intervention as planned.
Area IV: Evaluation and Research
- Plan how to assess, find data collection tools, monitor results of objectives, and disseminate conclusions.
Area V: Advocacy
- Identify emerging health issues; advocate for policy or environmental change with influential leaders.
Area VI: Communication
- Develop and deliver effective messages to identified audiences.
Area VII: Leadership and Management
- Coordinate partnerships and coalitions; manage budgets and resources.
Area VIII: Ethics and Professionalism
- Operate within established ethical codes and promote the health education profession.
Health Educator Ethics
Ethical behavior is essential when working with individuals, especially vulnerable populations. Given that most individuals or groups that health educators work with are vulnerable. The National Coalition of Health Educators adopted a standard code of ethics as follows:
2020 Code of Ethics for the Health Education Profession
(Coalition for National Health Education Organizations (CNHEO), 2020)
Article I: Core Ethical Expectations
Health Education Specialists display personal behaviors that represent the ethical conduct principles of honesty, autonomy, beneficence, respect, and justice. The Health Education Specialist should, under no circumstances, engage in derogatory language, violence, bigotry, racism, harassment, inappropriate sexual activities, or communications in person or through the use of technology and other means.
Health Education Specialists respect and support the rights of individuals and communities to make informed decisions about their health as long as such choices pose no risk to the health of others.
Health Education Specialists are truthful about their qualifications and the qualifications of others whom they recommend. Health Education Specialists know their scope of practice and the limitations of their education, expertise, and experience in providing services consistent with their respective levels of professional competence, including certifications and licensures.
Health Education Specialists are ethically bound to respect individuals' and organizations' privacy, confidentiality, and dignity. They respect the rights of others to hold diverse values, attitudes, and opinions. Health Education Specialists are responsible for engaging in supportive relationships that are free of exploitation in all professional settings (such as with clients, patients, community members, students, supervisees, employees, and research participants.)
Health Education Specialists openly communicate with colleagues, employers, and professional organizations when they suspect unethical practices that violate the profession's Code of Ethics.
Health Education Specialists are conscious of and responsive to social, racial, faith-based, and cultural diversity when assessing needs and assets, planning and implementing programs, conducting evaluations, and engaging in research to protect individuals, groups, society, and the environment from harm.
Health Education Specialists should disclose conflicts of interest in professional practice, research, evaluation, and dissemination.
Article II: Ethical Practice Expectations
Section I. Responsibility to the Public
Health Education Specialists are responsible for educating, promoting, maintaining, and improving the health of individuals, families, groups, and communities. When a conflict of issue arises among individuals, groups, organizations, agencies, or institutions, Health Education Specialists must consider all issues and give priority to those that promote the health and well-being of individuals and the public while respecting both the principles of individual autonomy, human rights, and equity as long as such decisions pose no risk to the health of others.
Section II. Responsibility to the Profession
Health Education Specialists are responsible for their professional behavior, the reputation of their profession, the promotion of certification for those in the profession, and the promotion of ethical conduct among their colleagues.
Section III. Responsibility to Employers
Health Education Specialists are responsible for their professional behavior in the workplace and for promoting ethical conduct among their colleagues and employers.
Section IV. Responsibility for the delivery of Health Education/Promotion
Health Education Specialists deliver evidence-informed practices with integrity. They respect all people's rights, dignity, confidentiality, inclusivity, and worth by using strategies and methods tailored to the needs of diverse populations and communities.
Section V. Responsibility in Research and Evaluation
Through research and evaluation activities, Health Education Specialists contribute to the health of populations and the profession. When planning and conducting research or evaluation, Health Education Specialists abide by federal, state, and tribal laws and regulations, organizational and institutional policies, and professional standards and ethics.
Section VI. Responsibility in Professional Preparation and Continuing Education
Those involved in the professional preparation and training of Health Education students and continuing education for Health Education Specialists must provide a quality education that meets professional standards and benefits the individual, the profession, and the public.
The 2020 Code of Ethics provides guidelines for ethical conduct in health education. The Areas of Responsibilities, Competencies, and Sub-Competencies for Health Education help form the basis of your future courses' content in the public health degree at BYU-Idaho.
W05 Study: Community Improvement Models
Overview
Purpose: Learn about the different planning models used in the public health field. Gain a basic understanding of how organizations employ these planning models to make changes in their communities.
Planning Models
History of Health Education
Earlier in the course, you learned about the history of public health. Planning models have been used throughout the history of public health and have evolved throughout the years. Planning models help you as a health professional to plan, implement, and evaluate programs in your profession.
Many different planning models exist. Perhaps the most famous is the PRECEDE-PROCEED Model.
PRECEDE-PROCEED Model
The PRECEDE-PROCEED planning model is the most authoritative for complex projects or when the general public is unaware of how to address the health problem. Marshall Kreuter and Larry Green developed it. Most planning models are based on the constructs in PRECEDE-PROCEED.
(Crosby & Noar, 2011a, 2011b)
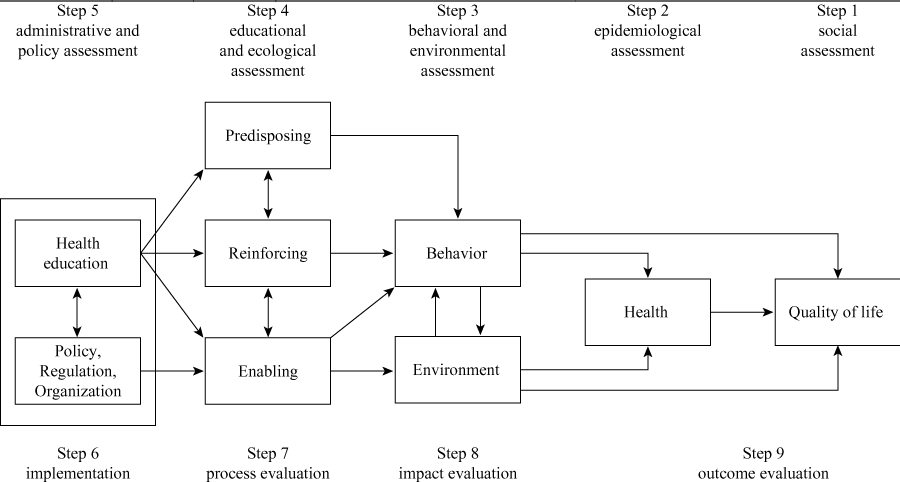
Access the appendix for a description of the image.
PRECEDE stands for Predisposing, Reinforcing, and Enabling Constructs in Educational Diagnosis and Evaluation. It involves assessing the following community factors:
Social assessment: Determine a given population's social problems and needs and identify desired results.
Epidemiological assessment: Identify the health determinants of the identified problems and set priorities and goals.
Ecological assessment: Analyze behavioral and environmental determinants that predispose, reinforce, and enable the identified behaviors and lifestyles.
Identify administrative and policy factors influencing implementation and match appropriate interventions to encourage desired and expected changes.
Implementation of interventions.
PROCEED stands for Policy, Regulatory, and Organizational Constructs in Educational and Environmental Development. It involves the identification of desired outcomes and program implementation:
Implementation: Design intervention, assess the availability of resources, and implement the program.
Process Evaluation: Determine if the program is reaching the targeted population and achieving desired goals.
Impact Evaluation: Evaluate the behavior change.
Outcome Evaluation: Identify if there is a decrease in the incidence or prevalence of the identified negative behavior or an increase in identified positive behavior.
Generic Planning Model
This course will use a simpler generic planning model, summarized below. Most public health programs should follow these or similar steps:
Understand your problem
Conduct a needs assessment
Set goals
Develop an intervention
Implement the intervention
Evaluate the results
Future Study
You will do a more in-depth study of the models introduced in this course in PUBH 390: Program Planning and Implementation.
Community Planning
Making a plan
Imagine you are planning a trip from your home to a distant city. There are many different methods of travel and many other routes to your destination. You could travel by plane, train, or by car. The plan you develop depends on your money, time, and options constraints. Planning in public health faces many of the same constraints.
What does planning look like in public health?
When addressing community health issues, public health planners must have a plan. Just having a good idea is not enough to successfully reduce health problems. One of the Eight Areas of Responsibility for health educators is planning health interventions. Like the example above, many different paths can be taken to reach the final destination; planning models will help find the best path.
SWOT
SWOT analysis and the Market Process are two tools that can be used to develop a community health plan.
A common approach when looking at issues in your community is to use a strategic planning technique. The Strengths, Weaknesses, Opportunities, and Threats (SWOT) analysis method is often used in business planning.
(Centers for Disease Control and Prevention, 2022)
Strengths: Internal positive attributes of the community that can facilitate activities.
Weaknesses: Internal attributes of the community that may hinder achieving its activities and goals.
Opportunities: External conditions that may facilitate community activities.
Threats: External conditions that may stand in the way of community activities.
Marketing Process
Using market research (input from the population) is an essential tool in determining the needs and wants of the target population.
Use market research to determine the needs and desires of the current and future clients in the target population.
Develop a product that satisfies the needs and desires of the clients.
Develop communication that informs and persuades the clients.
Ensure the product is provided appropriately, at the right time and place, and the right price.
Keep the clients satisfied and loyal after receiving the product.
Optional Resource:
Market_Segmentation.pdf (byui.edu)Mental Practice Exercise
Consider the following issue:
As a community health worker for the local health department, you are aware that cancers of all kinds (childhood blood cancers, brain tumors, lung cancer, skin cancer, prostate cancer, and breast cancer) take a significant toll on your community. You have just been given a large sum of money to reduce cancer in your community over the next five years.
In your mind, consider the following questions when developing a plan:
How will you do it?
What interventions will you implement?
How will you organize your work over the next five years?
How will you know if you are successful?
What populations will you target?
How will you get the interventions to those populations?
APA Format
Headings
Headings and Headers are two different parts of APA formatting. Headings are discussed in more detail below and you are not required to have a header on Term Paper assignments.
There are five levels of heading in the APA style. You are only expected to understand level 1 and 2 headings in this course. Try to avoid having only one subsection heading within a section. Do not label headings with numbers or letters. Always double-space your headings. Do not switch to single spacing for headings of any level. Do not add blank lines above or below headings, even if the heading falls at the bottom of the page.
Level 1 Headings: Level 1 is the highest or main heading level. Level 1 headings are centered, bold, and in title case. The text below this level of heading begins as a new paragraph.
Level 2 Headings: Level 2 headings are left justified, bolded, and use title case.

See the appendix for a description of the image.
The first paragraphs of any paper are always considered to be introductory. They do not need a heading. The title at the top of the page acts as the heading for your introduction.
Conclusion
The concluding paragraph(s) appear at the end of the body section. The conclusion does not need a heading of “Conclusion” and includes information about your findings or conclusions.
When writing your conclusion, restate your topic and why it is important. Restate your thesis and give an overview of future research possibilities.
Rough Draft
When you have finished writing your conclusion, you will turn in your rough draft. A rough draft is the first version of your paper and will need a lot of editing and revising. It is important to remember that your rough draft is a long way from your final draft, but it is your complete paper ready for editing and revisions, which we will discuss in next week's reading.
References
American Psychological Association. (n.d.). Headings. American Psychological Association. https://apastyle.apa.org/style-grammar-guidelines/paper-format/headings
Centers for Disease Control and Prevention. (2022, November 22). Do a SWOT Analysis. Centers for Disease Control and Prevention. https://www.cdc.gov/publichealthgateway/phcommunities/resourcekit/evaluate/do-a-swot-analysis.html?CDC_AA_refVal=https%3A%2F%2Fwww.cdc.gov%2Fphcommunities%2Fresourcekit%2Fevaluate%2Fswot_analysis.htmlhttps://www.nchec.org/responsibilities-and-competencies
Coalition for National Health Education Organizations (CNHEO). (2020, February). Code of Ethics for the Health Education Profession. National Comission for Health Education Credentialing. https://www.nchec.org/code-of-ethics
Crosby, R., & Noar, S. (2011a). PRECEDE-PROCEED. RHIhub. https://www.ruralhealthinfo.org/toolkits/health-promotion/2/program-models/precede-proceed
Crosby, R., & Noar, S. M. (2011b). What is a planning model? An introduction to PRECEDE-PROCEED: An introduction to PRECEDE-PROCEED. Journal of Public Health Dentistry, 71, S7–S15. https://doi.org/10.1111/j.1752-7325.2011.00235.x
Merriam-Webster. (2023). Merriam-Webster Dictionary. Merriam-Webster. https://www.merriam-webster.com/
National Commission for Health Education Credentialing, Inc. (n.d.). Responsibilities and Competencies for Health Education Specialists. NCHEC. https://www.nchec.org/responsibilities-and-competencies



This content is provided to you freely by BYU-I Books.
Access it online or download it at https://books.byui.edu/pubh_240_readings/chapter_5_community_improvement_planning.