Chapter 2: Needs Assessment, Part 2

Vocabulary
Community asset: A community asset or resource is anything that can be used to improve the quality of community life.
Construct: Concepts that have been refined and tested and are components of theories.
Enabling factors: Factors that can support or distract from change, like resources or skills.
Predisposing factors: Factors that can either support or distract from motivation to change, like attitude or knowledge.
Reinforcing factors: Factors that help sustain motivation and change by giving feedback or rewards.
Strategic issues: Fundamental policy choices or critical challenges that must be addressed for a community to achieve its vision.
Chapter 2: Planning Models and Needs Assessment, Part 2
This chapter presents some examples of how others have planned health programs, using specific planning models that have been developed by public health professionals. Planning models help ensure that public health interventions are based on a solid foundation. They provide a basic framework that helps us structure our planning, implementation, and evaluation efforts related to the program we deliver in a community.
We will review four of the most common planning models used currently in public health:
PRECEDE-PROCEED
MAPP
MAP-IT
Healthy Cities/Healthy Communities
NOTE: For the Course Project you will develop a Grant Application for a hypothetical program, following similar steps in a generalized planning model.
PRECEDE-PROCEED
(CTB, n.d.-a)
What Is PRECEDE-PROCEED?
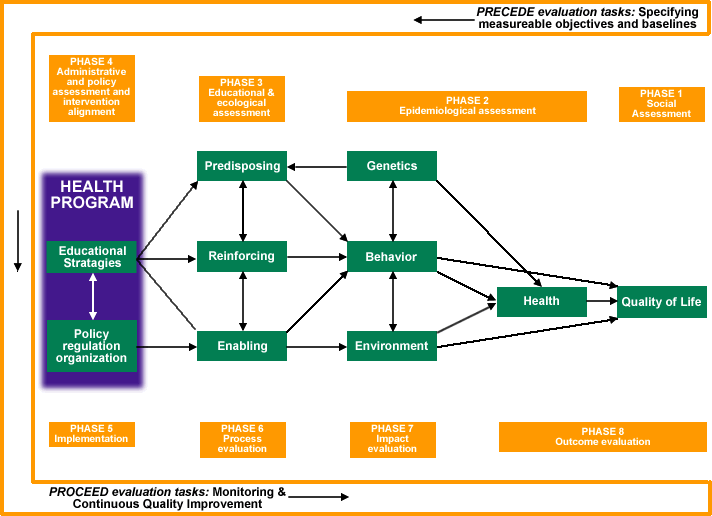
This planning model was developed for public health and can be applied to other community improvement projects as well. Addressing the phases suggested by this model ensures that all necessary steps are taken in formulating, implementing and evaluating an intervention.
(Green & Kreuter, 2005)
Access the appendix for a description of the image
PRECEDE stands for Predisposing, Reinforcing, and Enabling Constructs in Educational/Environmental Diagnosis and Evaluation. It represents the process that precedes, or leads up to, an intervention.
PROCEED spells out Policy, Regulatory, and Organizational Constructs in Educational and Environmental Development. It describes how to proceed with the intervention itself.
How To Use PRECEDE-PROCEED
The eight phases are described here, as well as a brief example of using this model.
PRECEDE is the diagnostic portion of the model. It starts with the idea that the focus of change must be on its desired outcome and works backward from that outcome to construct an intervention that will bring it about. It has four phases:
Phase 1: Social diagnosis – Determine what the community wants and needs to improve its quality of life.
Phase 2: Epidemiological diagnosis – Determine the health problems or other issues that affect the community’s quality of life. Include the behavioral and environmental factors that must change in order to address these problems or issues. Behavioral factors include patterns of behavior that constitute lifestyles. In considering environmental factors, you should include the physical, social, political, and economic environments.
Phases 1 and 2 identify the goals of the intervention.
Phase 3: Educational and organizational diagnosis – Determine what to do in order to change the behavioral and environmental factors in Phase 2, taking into account predisposing factors (knowledge, attitudes, beliefs, values, and confidence); enabling factors (availability of resources, accessibility of services, government laws and policies, issue-related skills); and reinforcing factors (largely the influence of significant others in the social environment).
Phase 4: Designing programs or interventions and the support for them through administrative and policy diagnosis – determine (and address) the internal administrative and internal and external policy factors that can affect the success of your intervention. Administrative factors are organizational structure, procedures, culture, and resources; policy factors are both internal policies and funders’ requirements, oversight agency regulations, state or federal laws, local ordinances, and unstated community policies.
Phases 3 and 4 set the structure and targets for the planning and design of the intervention.
PROCEED is the treatment portion of the model, and comprises the implementation and evaluation of the intervention. It consists of four phases:
Phase 5: Implementation – Conduct the intervention.
Phase 6: Process evaluation – Determine whether the intervention is actually taking the actions intended.
Phase 7: Impact evaluation – Determine whether the intervention is having the intended effects on behaviors and/or environment.
Phase 8: Outcome evaluation – Determine whether the intervention brings about the improvements in quality of life identified by the community.
An important part of the model is that your plan or intervention should be revisited and revised, based on continued analysis and the results of the various evaluations.
Brief Example of a Health Program Using PRECEDE-PROCEED
PRECEDE:
Phase 1: Social diagnosis
Surveys and town meetings reveal that people in this community want to reverse the recent trend of increasing rates of obesity and overweight.
Phase 2: Epidemiological diagnosis
Data from surveys and area agencies show that residents eat few fruits and vegetables and have few places to exercise.
Phase 3: Educational and organizational diagnosis
Coalition brings together leaders, agencies and key community members who set goals of developing community gardens, walking trails, and bike paths.
Phase 4: Design of interventions
Coalition subcommittees plan with local agricultural agencies to set up two new community gardens and meet with city park & recreation officials to develop walking trails and bike paths. Coalition sets a budget and timeline, recruits volunteers and publicizes the projects.
PROCEED:
Phase 5: Implementation
Development begins of community gardens, walking trails, and bike paths, following the timeline that was set by committees.
Phase 6: Process Evaluation
Leaders evaluate: How are the committees working together? How are the gardens, trails, and paths progressing?
Phase 7: Impact Evaluation
Leaders evaluate: Are people using the garden produce? Are walkers and bikers using the trails and paths?
Phase 8: Outcome Evaluation
Final evaluation: Have residents’ fruit and vegetable consumption increased? Has physical activity increased? After years of the project, have rates of obesity and overweight leveled or decreased?
MAPP: Mobilizing for Action through Planning and Partnerships
(CTB, n.d.-b)
Access the appendix for a description of this image
What Is MAPP?
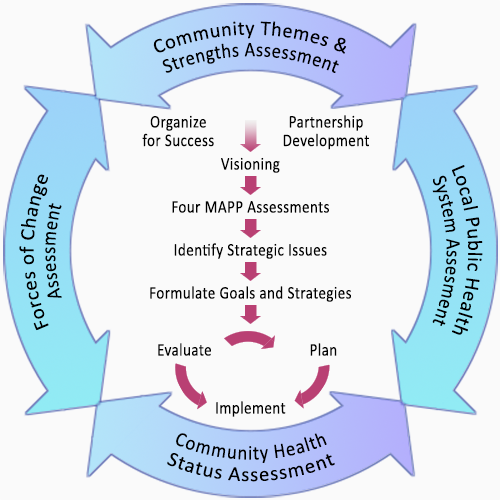
Mobilizing for Action through Planning and Participation (MAPP) is a model for developing a healthy community. Its community perspective addresses the community as a whole and makes it flexible enough to be used with any community system. Its basic philosophy is broad community participation in planning and implementation of the initiative.
Why use MAPP?
Compared to other models, the Assessment Phase of MAPP is especially thorough and includes community themes and strengths as identified by community members, the state of the local public health system, the state of the community’s health status, and real or potential forces of change. MAPP uses systems thinking to analyze these assessments, identify key issues, and develop strategies for addressing them.
If properly realized, MAPP can permanently improve the ways in which individuals and organizations relate and the extent to which the community can control its own health and quality of life.
How To Use MAPP
The six phases are described here, as well as a brief example of using this model.
Phase 1: Organize for Success/Partnership Development
Determine the necessity of undertaking the MAPP process.
Identify and organize participants.
Determine the resources you will need for the planning process.
Make sure the community is ready to conduct a successful planning process.
Develop a management structure for the process: agree on ground rules, assemble a work plan, and designate the coordinator.
Phase 2: Visioning
Identify other visioning efforts and make connections with other groups.
Design the visioning process and its management: either by the whole community or a representative advisory committee.
Conduct the visioning process, then keep the vision and values alive throughout the MAPP process.
Phase 3: The Assessments
Community Themes and Strengths: Thoughts, opinions, concerns, and assets.
Local Public Health System Assessment (LPHSA) uses the National Public Health Performance Standards Program, based on the Ten Essential Public Health Services.
Community Health Status Assessment addresses health and quality of life to summarize major health issues.
Forces of Change Assessment identifies current and anticipated factors that directly or indirectly affect health.
Phase 4: Strategic Issues
Brainstorm potential strategic issues, starting with the MAPP vision.
Why is the issue strategic and how does it affect the vision?
What are the consequences of not addressing the issue?
Consolidate related or overlapping issues.
Prioritize by arranging issues into an ordered list, which will grow into your action plan.
Phase 5: Goals and Strategies
Develop goals related to the vision and strategic issues.
Generate strategy alternatives.
Consider details and barriers to implementation.
Select and adopt strategies.
Draft a planning report that will be a roadmap for the project and a document to inform the community about the process.
Celebrate the completion of the planning phase, to energize participants and create interest and support in the community.
Phase 6: Action Cycle
A. Plan for action: Organize, develop objectives, and establish accountability. Objectives need to be specific, measurable, achievable, relevant, timed, and challenging.
B. Implementation: Review action plans, then implement and monitor.
C. Evaluation: Prepare at the beginning of the MAPP process, focus the evaluation design, gather credible evidence, and justify the conclusions.
D. Share lessons learned and celebrate successes.
E. Maintain the cycle to continue improving.
Brief Example of Using the MAPP Model:
Phase 1: Organize for Success/Partnership Development
The community decides they need the MAPP process to address several recent health issues. A coalition is formed of local agencies and concerned individuals. They agree on a series of planning meetings, set ground rules, and choose a coalition leader.
Phase 2: Visioning
The coalition invites the whole community to participate, and together they identify the vision of a healthier community for all residents with values of respect, inclusion, and communication.
Phase 3: The Assessments
The coalition conducts the four recommended assessments. Results show several health issues of concern including teen tobacco use, childhood obesity, drug overdoses, heart disease, and skin cancer.
Phase 4: Strategic Issues
The coalition considers all potential health issues to address, according to the established vision and values. They identify the two highest priorities as teen tobacco use and childhood obesity.
Phase 5: Goals and Strategies
The coalition forms subcommittees which develop goals and strategies. The Tobacco Committee identifies the long-term goal of reducing the rate of teen tobacco use. Strategies include enforcing and monitoring local ordinances that restrict tobacco sales to minors. The Childhood Committee sets a long-term goal of leveling the increase in rate of childhood obesity. Strategies include incorporating lesson plans in elementary schools for games and activities to include healthier snacks and limiting sweet beverages. The coalition develops a report of the plans, and publicizes it through a community newsletter and on their Facebook page, highlighting the work of the two committees.
Phase 6: Action Cycle
A. The committees form short-term objectives. The Tobacco committee decides the town will hire two monitors who will check ten stores each month for compliance with laws restricting tobacco sales to minors. The Childhood Committee decides two health educators will present one healthy snack lesson per month to each class in the elementary school.
B. Both committees implement their plans and report back to the coalition.
C. The coalition surveys participants. Tobacco compliance was only 30% the first month but has risen to 70% by the second month as the retail stores became aware of the monitoring process. In schools the pre- and post-tests at healthy snack lessons indicate children are now 80% more willing to include carrots and apple slices for snacks.
D. The coalition reviews lessons learned: stores know they are being checked and may pretend to comply. Children in schools may not actually consume healthier snacks. The Tobacco Committee decides to make the compliance checks more unexpected. The Childhood Committee decides to budget for food samples at the snack lessons.
E. Both committees continue the cycle of modifying their short-term objectives and reporting progress to the coalition.
MAP-IT
(CTB, n.d.-c)

What is MAP-IT?
The MAP-IT framework is designed to help communities develop local health initiatives. Its phases provide a logical structure to address and resolve local health problems and to build healthy communities. The phases include the following:
M—Mobilize individuals and organizations that care about the health of your community into a coalition.
A—Assess the areas of greatest need in your community, as well as the resources and other strengths that you can tap into to address those areas.
P—Plan your approach: Start with a vision of where you want to be as a community, then add strategies and action steps to help you achieve that vision.
I—Implement your plan using concrete action steps that can be monitored and will make a difference.
T—Track your progress over time.
Why Use MAP-IT?
MAP-IT emphasizes integrating all stakeholders in a widely-supported, community-owned effort. The efforts start with an assessment of health needs and what resources are available in the community. Plans are developed with timelines, objectives, and action steps. MAP-IT allows for adjustment of plans, according to the ongoing evaluation process.
How To Use MAP-IT
The five steps are described here, as well as examples of how the steps in this model have been used.
Step 1: Mobilize
Gather key individuals and agencies into a coalition. Aim for broad representation. Engage potential coalition members around issues that are already of concern in the community. Create a vision. Brainstorm potential partners from among likely stakeholders, involving as many different community sectors as possible.
Step 2: Assess
Identify real health needs of the community, not just impressions. Gather data about major health issues. Also, identify assets and resources of the community and what it has to offer.
Step 3: Plan
Create an action plan with concrete steps and deadlines. Assign responsibility of what exactly is to be achieved, by whom and by when. Include ongoing data collection for monitoring progress. Create a timeline. Include a communication plan of how to keep the community informed of the projects.
Step 4: Implement
Complete assigned tasks according to the plan and timeline. Publicize the efforts in the community. Showcase the accomplishments and acknowledge partners.
Step 5: Track
Conduct regular evaluations to measure progress over time and report back to the coalition.
Examples of How MAP-IT has Been Used:
Mobilization
One state formed a partnership with a group of individuals representing a broad sector of both public and private organizations, including members from local departments of health. This group was charged with the responsibility of meeting the state’s public health improvement goals.
Assessment
One coalition determined priority health issues through its steering committee, which evaluated health data, sought expert opinions, invited public comments, and conducted an opinion survey of residents. They used a consensus method to limit the scope of its objectives to four priority health areas and four disease risk factors. The four priority health areas included alcohol and drug abuse, cancer, heart disease, HIV and other sexually transmitted diseases. The focal risk factors were lack of access to preventive care, tobacco use, poor nutrition, and lack of physical activity.
Planning
To achieve its year 2030 objectives, one health department initiated a Worksite Wellness Council. They focused on increasing health promotion and disease prevention activities in work sites, where most adults spend the majority of their time. The Council set a goal of having 20 percent of its workforce in sites certified by a national Worksite Wellness agency.
Implementation
The Office of Healthy Residents in one area is responsible for keeping their Healthy People initiative on track. Staff are available for support and training, particularly coalition building. There is also a mayor’s task force that certifies communities in the Healthy People project. The communities do an assessment and then implement an action plan.
Tracking Example
One health department’s statistical and program staff assessed progress and analyzed trends. Based on their trend analysis, staff categorized each objective as “likely to be achieved,” “unlikely to be achieved,” or “uncertain.” They then continued to monitor all objectives and made them part of annual reports.
Healthy Cities/Healthy Communities
(CTB, n.d.-d)
Access the appendix for a description of the image
What Is Healthy Cities/Healthy Communities?
(World Health Organization, n.d.-a)
"Health is created and lived by people within the settings of their everyday life; where they learn, work, play, and love" (WHO, 1986, p. 4).
This statement is at the heart of the Healthy Settings approach, which has its roots in the WHO Health for All strategy and, more specifically, the Ottawa Charter for Health Promotion. Initiated by WHO in 1986, Healthy Cities have spread rapidly across the world.
A Healthy City aims to do the following:
Create a health-supportive environment
Achieve a good quality of life
Provide basic sanitation and hygiene needs
Supply access to health care
Being a Healthy City depends not only on health infrastructures, but also on a commitment to improve a city's environs and a willingness to forge the necessary connections in political, economic, and social arenas.
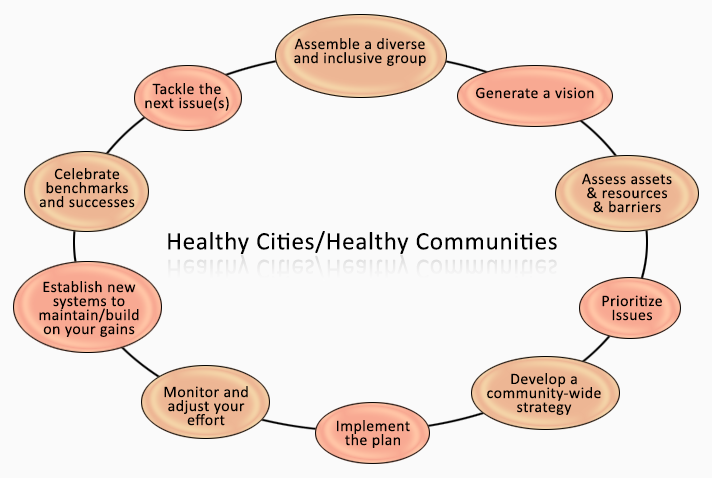
Healthy Cities/Healthy Communities is now used as a philosophical framework for an inclusive, participatory process aimed at raising the quality of life for everyone and creating a truly healthy community.
There are two basic premises underlying the Healthy Cities/Healthy Communities concept. The first is a comprehensive view of health and community issues, which covers a broad range of factors that contribute to a healthy community. The second is a commitment to the active promotion of a healthy community, rather than the treatment of problems.
Communities can foster citizen empowerment and equity by addressing the social and other determinants of health and community issues (including the Ottawa Charter’s list of peace, shelter, education, food, income, stable ecosystem, sustainable resources, social justice, and equity), and by creating appropriate policy and environments, encouraging social action, providing personal skills, and reorienting services to a more wide-ranging approach.
Why use Healthy Cities/Healthy Communities?
Its community perspective leads to local ownership of the efforts, due to participation in development and implementation. Broader ideas are gained from a participatory process.
Access to citizens’ knowledge of the community helps to avoid pitfalls caused by ignorance of community history and relationships.
Community assets and resources are identified to take advantage of what already exists.
A healthy community self-image is fostered with a commitment to the process of improving health.
While a Healthy Cities/Healthy Communities process should involve everyone, some particularly important participants include local government and officials; those affected by the issue(s); those who will actually administer and implement the initiative, or whose lives or jobs will be affected by it; any organizations that will be expected to work together; and opinion leaders.
How To Use Healthy Cities/Healthy Communities
There is no step-by-step procedure. Both the content and the structure of the process depend upon your community’s needs and on community decisions.
The 10 important components of a Healthy Cities/Healthy Communities process are as follows:
Create a compelling vision: Define the efforts to be made based on shared values.
Embrace a broad definition of health and well-being as not just physical health but including peace, shelter, education, income, food, stable ecosystem, sustainable resources, social justice, and equity.
Address quality of life for all groups and communities.
Engage diverse citizen participation and be citizen-driven. Include participants from all racial, ethnic and socio-economic groups, and all walks of life.
Seek multi-sectoral membership and widespread community ownership. Include all sectors of the community – government, the business and non-profit communities, health care, education, faith communities, cultural institutions and the arts, target populations, and ordinary citizens
Acknowledge the social determinants of health and the interrelationship of health with other issues (housing, education, peace, equity, social justice).
Address issues through collaborative problem-solving. Conflicts should be viewed as opportunities, and people should be helped to work together to reach creative solutions.
Focus on change of systems, the ways in which the community operates, and the attitudes, assumptions, and policies behind the way the community operates.
Build capacity using local assets and resources. All communities have real and potential strengths that should be identified and included in a Healthy Cities/Healthy Communities effort.
Measure and benchmark progress and outcomes. Monitor and evaluate the effort to be sure that it’s effective. Regularly monitoring what you’re doing allows you to spot and correct inadequacies in goals, methods, and communication before they derail your initiative.
Examples of WHO’s efforts in Healthy Cities/Healthy Communities:
Improving Health Literacy
(WHO, n.d.-b)
By improving people’s access to health information and their capacity to use it effectively, health literacy becomes critical to empowerment. Improving health literacy in populations provides the foundation on which citizens are enabled to play an active role in improving their own health, engage successfully with community action for health, and push governments to meet their responsibilities in addressing health and health equity. Meeting the health literacy needs of the most disadvantaged and marginalized societies will particularly accelerate progress in reducing inequities in health and beyond.
Mozambique
(WHO, n.d.-c)
60-year-old Raquelina Mazuze is proud of her contribution to the fight against polio as a social mobilizer in her native Mozambique. Following the recent outbreak of wild poliovirus type 1 in the country, she has been helping to prepare her community for a forthcoming vaccination drive, which aims to protect nearly four million children in the four most at-risk provinces. Having been involved in the health sector for decades, Raquelina also spends her days encouraging older people around her to stay active, eat healthily, and to keep serving their community, just as she does.
Partners commit to improve Maternal, Newborn and Child Health
(WHO, 2023)
At a meeting of the Network for improving quality of care for Maternal, Newborn and Child Health (MNCH) held in Accra, Ghana, ten global partners resolved to strengthen collaboration towards improving maternal, newborn, and child health through sustained quality of care at all levels of the health system. This meeting was aimed at engaging with the champions from the government and implementing partners and other stakeholders to build on five years of efforts to integrate quality of care in health systems and maternal, newborn, and child health interventions.
Needs Assessment, Part 2: Setting Priorities
[Note: This will be used in Section 1, Steps 6-12 of the Term Project]
In Chapter 1, we introduced the need for gathering data about the community. In most cases long lists of problems will be identified, and the next critical step is deciding which are most important and realistic to address first.
There are many ways to do this, and members of any given sample community (priority population and stakeholders) should be involved in helping us identify what health issues should be focused on. The constraints of the project have been set: we have one year and $100,000 to develop a public health intervention to address health concerns in this community.
For consensus building, we can meet with the stakeholders to review the data collected and come to an agreement of what health issue should be focused on. It’s important that decision makers, funders, and those in the community that would be impacted by the program are a part of the decision-making process.
We also need to identify the underlying causes of the health issue. We need to look at the many variables that can influence the health issue. Then we can focus our program on one underlying cause of the health issue that has been identified.
Analyzing Community Problems
(CTB, n.d.-e)
Below are some criteria you may consider when prioritizing community problems:
The problem occurs too frequently (frequency)
The problem has lasted for a while (duration)
The problem affects many people (scope or range)
The problem is disrupting to personal or community life, and possibly intense (severity)
The problem deprives people of legal or moral rights (equity)
The issue is perceived as a problem (perception)
This last criterion, perception, can also help indicate readiness for addressing the issue within the community. What is seen as a problem can vary from place to place and group to group in the same community.
How Should I Analyze a Community Problem?
The goal is to understand the problem better and to deal with it more effectively. Here are some steps to follow:
1. Justify the choice of the problem.
Apply the criteria – frequency, duration, range, severity, equity, perception – as well as asking yourself whether the problem is one that you should focus on, or not.
2. Frame the problem.
(CTB, n.d.-f)
State the problem without implying a solution or blaming anyone.
3. Identify what behavior and environmental factors need to change for the problem to be solved.
This can be as simple as individuals changing their behavior or as complex as persuading legislators to change laws or the environment.
4. Analyze the root causes of the problem.
(CTB, n.d.-g; Lopez, n.d.)
[Note: This will be used in Section 1, Step 9 of the Term Project]
The real cause of a problem may not be immediately apparent. It may be a function of a social or political system, or it may be rooted in a situation that seems unrelated. One method to discover the root cause is the “But Why?” technique. This technique consists of stating the problem as you perceive it and asking “But why?” Then answer that and ask again, “But why?”
Example: There are too many children in the community who are overweight or obese.
The problem is particularly serious among low-income families. (But why?)
Because many low-income children don’t eat a healthy diet and don’t exercise enough. (But why?)
Because their parents may not have the knowledge of healthy foods and have access only to fast food. Kids don’t play outside because it’s too dangerous. (But why?)
Parents may never have been exposed to nutrition. Low-income neighborhoods are unprofitable places to do business. The streets are dangerous because there are few job opportunities in the community, and young men turn to making money in any way possible.
You may begin to think about advocacy to bring supermarkets to low-income neighborhoods, after-school programs for physical exercise, or parent nutrition education or anti-gang programs. Continued questioning may reveal deeper causes that your organization can tackle.
5. Identify the restraining and driving forces that affect the problem.
(Nagy, n.d.)
This is called a force field analysis, looking at the restraining forces that keep the problem from changing (social structures, cultural traditions, and so on) and the driving forces that push it toward change (policy change, ongoing public education efforts, and so on).
Forces restraining change. This example would include the following:
The desirability of junk food – kids like it because we’re programmed to like fat, salt, and sugar, which are freely available.
Reluctance of chains to open food stores in low-income neighborhoods.
The domination of the streets by gangs and drug dealers.
Some forces driving change might be:
Parents’ concern about their children’s weight.
Children’s desire to participate in sports or simply to be outdoors.
Media stories about childhood obesity and its consequences for children.
6. Find any relationships between the issue of concern and others in the community.
Other problems may stem from the same root cause, so you could partner with other organizations on similar issues.
7. Identify personal factors that may contribute to the problem.
(CTB, n.d.-h)
Whether the problem involves individual behavior or community conditions, those affected by it bring a whole collection of genetics, knowledge, beliefs, background, and assumptions about the world. These might contribute to the problem or to its solution.
A few examples:
Genetic predisposition for diabetes and other conditions.
Lack of knowledge about healthy nutrition.
Lack of knowledge or skills for preparing healthy foods.
8. Identify environmental factors that may contribute to the problem.
These might include the lack of services and other support, accessibility to information, the social and financial costs and benefits of change, and other conditions.
Sample environmental factors:
Poverty.
Hopelessness and lack of employment in low-income neighborhoods.
Lack of availability of healthy food in low-income neighborhoods.
Availability of snack foods high in salt, sugar, and fat.
Media bombardment about unhealthy snacks, drinks, and fast food.
9. Identify targets and agents of change for addressing the problem.
(CTB, n.d.-i)
The point of this step is to understand where and how to direct your work most effectively.
Targets of change:
Parents and children in low-income neighborhoods.
School teachers and those responsible for school food programs.
Executives of supermarket chains.
Gang members and youth at risk of becoming gang members.
Potential agents of change:
Parents as controllers of their children’s diets.
School administrators responsible for food programs.
Local officials who could create incentives for markets in underserved neighborhoods.
Recreation departments and other agencies that might create safe physical activity programs for children.
Community hospitals, clinics, and private medical practices.
Public relations offices of national or regional fast food restaurant chains.
This process will help you develop a strategic plan to reach the real causes of the problem and focus on the targets and agents of change most likely to improve the situation.
Some Decision-Making Processes
(CTB, n.d.-j)
1. Relative worth.
Each participant receives a fixed number of points (for example, 100 points). These points can be distributed among the items to be prioritized in whatever way the participant desires. Participants can distribute points in a number of ways:
Give all points to a single, very important item.
Distribute points evenly among all items (if none is more important than another).
Distribute some points to some items, no points to other items.
In the tabulation, items are given priority ranking according to the total points the group assigns.
2. Forced ranking.
Needs are ranked separately on a scale.
For example, if there are ten items, the most important item is assigned a “1,” the second most important item is assigned a “2,” and so on down to the least important item, which receives a “10.”
In the tabulation, the item that receives the lowest number of points is assigned highest priority, the item that receives the second lowest number of points receives second priority, and so on.
3. Delphi method.
The coordinating group assembles participants with knowledge and experience in the issue to be addressed.
Needs are identified and presented to participants for feedback. A deadline for returning responses is given.
The coordinating group records all responses and distributes them to participants.
Participants are asked to review the responses and add additional ideas or delete ones considered not important or not feasible. Participants then choose the three or five most important ideas and rank these in descending order of importance.
Results of the rankings are collated and analyzed.
Findings are returned to participants who are again asked to rank the top three or five preliminary priorities. Additional rounds may be implemented if necessary.
Results are collated and categorized. An overall ranking is determined.
Delphi enables participants to examine group responses with each succeeding round, and to alter their views or to provide a rationale for sustaining a divergent opinion.
4. Hanlon method. There are three central features of the method:
Focuses on identifying explicit criteria to be considered in setting priorities.
Ability to organize factors into groups that are weighted relative to each other.
Allows for modification and individual scoring of factors.
Criteria for scoring of factors and subsequent priority setting include the following:
Size of the problem.
Seriousness of the problem.
Estimated effectiveness of intervention(s) under consideration.
PEARL (Propriety, Economic Feasibility, Acceptability, Resource Availability, and Legality)
P = Propriety: Is an intervention suitable?
E = Economics: Does it make economic sense to address the problem?
A = Acceptability: Will this community accept an emphasis on this problem, and will they accept the proposed intervention?
R = Resources: Are resources available?
L = Legality: Do the current laws allow the intervention to be implemented?
5. Delbeq method.
The Delbeq "Two Step" method involves the use of a nominal group process to develop a detailed set of priority issues, and the subsequent sharing of issues and development of a consolidated list of priorities.
The term "nominal group" is used to underline the highly controlled dimension of the process.
In the first stage, participants are asked to privately record their major concerns on a sheet of paper.
Facilitators then go around the group to elicit their priority concerns. This is usually done anonymously, by asking for a limited list (2 or 3) of priority concerns to be handed in to facilitators. These are recorded on a white board.
An alternative is to hold a "round robin" where priority concerns are elicited from participants one at a time. No comments are permitted during this stage.
In the second stage, facilitators take participants through a controlled discussion; first to clarify priority concerns, and then to consolidate common issues.
Finally, for health planning efforts where large lists of priority concerns are typically generated, participants may go through a ranking process to limit the number of potential options.
6. Importance and Feasibility
(NACCHO, n.d.)
To make sure we are addressing problems that will yield the greatest results, we need to measure both importance and feasibility. This is especially useful in order to focus on areas that achieve maximum results with limited resources.
Factors to Consider while Prioritizing Issues:
Importance of Health Issue:
Prevalence and incidence
Comorbidities
Reduced quality of life
High likelihood of death
Feasibility of Intervention
Costs of treatment or intervention
Political will for support and funding
Adequacy of public health infrastructure
How realistic is prevention or mitigation
The table below is an example of an agency comparing potential projects. It could be used in a variety of ways, to identify a main priority health outcome to focus on, to prioritize which underlying factor to focus on, or to prioritize which strategy to choose.
Suggested Steps to Compare Projects:
List the health issues the community is facing in a table, as in the example below.
Consider each health issue and its underlying factors. Assign a score of 1 to 3 (1=Low, 2=Moderate, 3=High) for each activity and for both Importance and Feasibility.
Add scores in each row and compare totals.
Compare the scores in each category and note examples in the Table.
High Importance and High Feasibility (as in B below) – These are the highest priority items.
Low Importance and High Feasibility (as in C below) – Although they might be popular, they need to be reconsidered.
High Importance and Low Feasibility (as in D below) – Long term projects with potential but will require significant resources that can be overwhelming.
Low Importance and Low Feasibility (as in A below) – These are the lowest priority items and could give resources to higher priority items.
| Health Problems | Importance = | Feasibility = | Total |
A | Some rare cancers are on the rise. | 1 | 1 | 2 |
B | Diabetes prevalence is increasing. | 3 | 3 | 6 |
C | Some immigrants have high rates of infectious diseases. | 1 | 2 | 3 |
D | Childhood obesity has doubled. | 3 | 1 | 4 |
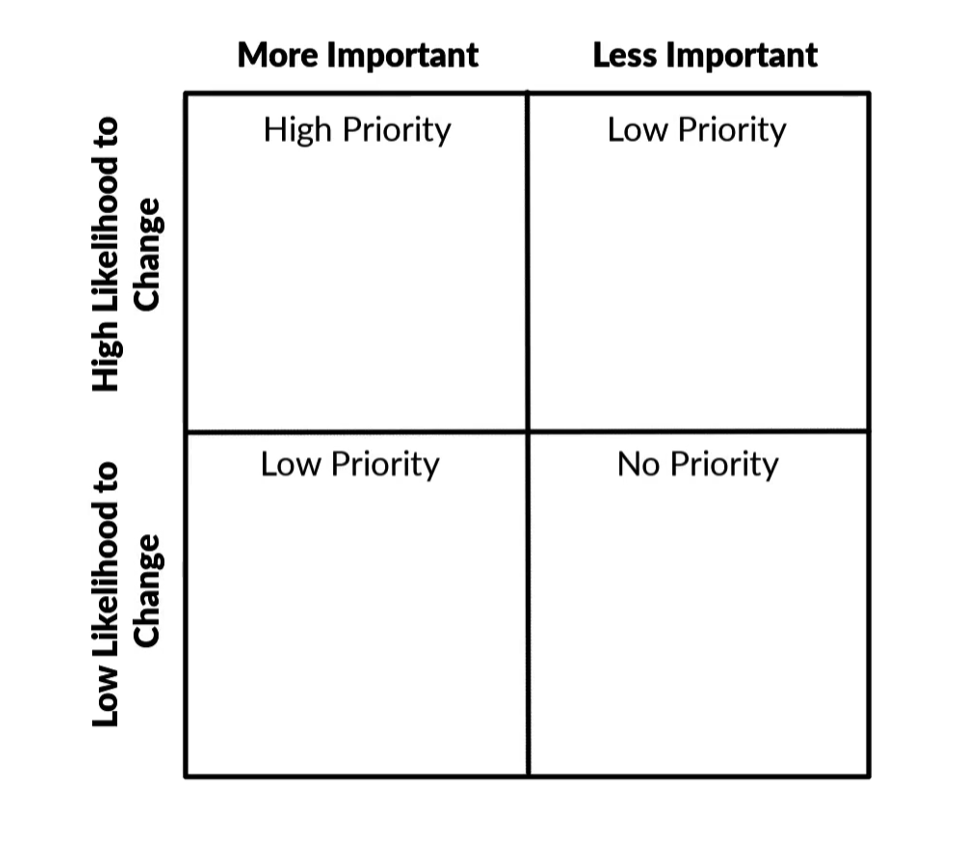
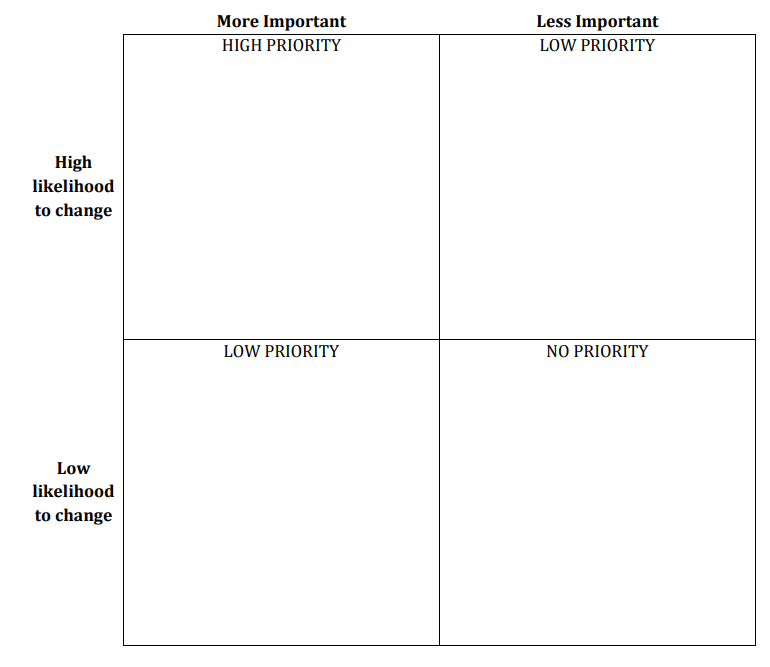
7. Prioritizing Causes Matrix
(MDH, n.d.)
Assessing Changeability: For each intervening variable, use this 2x2 table to help you prioritize your contributing factors. First, is your contributing factor important? To what degree does this contributing factor affect opioid misuse in your community? Next, how easy or difficult is it to bring about change in the contributing factor? Based on those two questions, place your contributing factor in one of these boxes. Whatever ends up in the most important and most changeable quadrant of the 2x2 matrix is your prioritized focus. You may need to run this prioritization process a few times to narrow down to the top contributing factors to focus on.
References
CTB. (n.d.-a). Chapter 2, Section 2. PRECEDE/PROCEED. Community Tool Box. https://ctb.ku.edu/en/table-contents/overview/other-models-promoting-community-health-and-development/preceder-proceder/main
CTB. (n.d.-b). Chapter 2, Section 13. MAPP: Mobilizing for Action through Planning and Partnerships. Community Tool Box. https://ctb.ku.edu/en/table-of-contents/overview/models-for-community-health-and-development/mapp/main
CTB. (n.d.-c). Chapter 2, Section 14. MAP-IT: A Model for Implementing Healthy People 2020. Community Tool Box. https://ctb.ku.edu/en/table-of-contents/overview/models-for-community-health-and-development/map-it/main
CTB. (n.d.-d). Chapter 2, Section 3. Healthy Cities/Healthy Communities. Community Tool Box. https://ctb.ku.edu/en/table-of-contents/overview/models-for-community-health-and-development/healthy-cities-healthy-communities/main
CTB. (n.d.-e) Chapter 3, Section 5. Analyzing Community Problems. Community Tool Box. https://ctb.ku.edu/en/table-of-contents/assessment/assessing-community-needs-and-resources/analyzing-community-problems/main
CTB. (n.d.-f). Chapter 32, Section 5. Reframing the Issue. Community Tool Box. https://ctb.ku.edu/en/table-of-contents/advocacy/encouragement-education/reframe-the-debate/main
CTB. (n.d.-g). Chapter 17, Section 2. Thinking Critically. (n.d.). Community Tool Box. https://ctb.ku.edu/en/table-of-contents/analyze/analyze-community-problems-and-solutions/think-critically/main
CTB. (n.d.-h). Chapter 19, Section 2. Understanding Risk and Protective Factors: Their Use in Selecting Potential Targets and Promising Strategies for Intervention). Community Tool Box. https://ctb.ku.edu/en/table-of-contents/analyze/choose-and-adapt-community-interventions/risk-and-protective-factors/main
CTB. (n.d.-i). Chapter 18, Section 3. Identifying Targets and Agents of Change: Who Can Benefit and Who Can Help. Community Tool Box. https://ctb.ku.edu/en/table-of-contents/analyze/where-to-start/identify-targets-and-agents-of-change/main
CTB. (n.d.-j) Chapter 3, Section 23. Developing and Using Criteria and Processes to Set Priorities. Community Tool Box. https://ctb.ku.edu/en/table-of-contents/assessment/assessing-community-needs-and-resources/criteria-and-processes-to-set-priorities/main
Green, L. and Kreuter, M. (2005). Health promotion planning: An educational and ecological approach (4th Ed.). Mayfield Publishers.
Lopez, C. (n.d.). Chapter 17, Section 4. Analyzing Root Causes of Problems: The “But Why?” Technique. Community Tool Box. https://ctb.ku.edu/en/table-of-contents/analyze/analyze-community-problems-and-solutions/root-causes/main
MDH. (n.d.). Deliverables. Maryland Department of Health. (n.d.). https://health.maryland.gov/bha/OMPP/Documents/DeliverablesandOMPP_NeedsAssessmentReport.pdf
NACHHO. (n.d.) Guide to Prioritization Techniques. National Association of County & City Health Officials, The National Connection for Local Public Health. https://www.naccho.org/uploads/downloadable-resources/Gudie-to-Prioritization-Techniques.pdf
Nagy, J. (n.d.). Chapter 17, Section 3. Defining and Analyzing the Problem. Community Tool Box. https://ctb.ku.edu/en/table-of-contents/analyze/analyze-community-problems-and-solutions/define-analyze-problem/main
WHO. (1986). The Ottawa Charter. World Health Organization. https://intranet.euro.who.int/__data/assets/pdf_file/0004/129532/Ottawa_Charter.pdf
WHO. (2023, March 23). Global partners commit to improve Maternal, Newborn and Child Health. World Health Organization. https://www.afro.who.int/countries/ghana/news/global-partners-commit-improve-maternal-newborn-and-child-health
WHO. (n.d.-a). Creating healthy cities. World Health Organization. https://www.who.int/activities/creating-healthy-cities
WHO. (n.d.-b). Improving Health Literacy. World Health Organization. https://www.who.int/activities/improving-health-literacy
WHO. (n.d.-c). Raquelina Mazuze, Mozambique, Social Mobilizer. World Health Organization. https://www.afro.who.int/about-us/making-difference-health-africa/raquelina-mazuze-social-mobilizer



This content is provided to you freely by BYU-I Books.
Access it online or download it at https://books.byui.edu/pubh_390_readings_2nd_edition_/chapter_2_needs_assessment_part_2.